We are developing the social individualist meta-context for the future. From the very serious to the extremely frivolous... lets see what is on the mind of the Samizdata people.
Samizdata, derived from Samizdat /n. - a system of clandestine publication of banned literature in the USSR [Russ.,= self-publishing house]
|
“Join thousands of Dryathletes dropping the drink this January and raising money to help beat cancer sooner”, says Cancer Research UK. What bilge. Abstaining from alcohol for a month does nothing and is nothing. Absent real problems, anyone can just drink exactly what they want whenever they want. That anyone takes seriously the pretence that deciding not to drink for a while is an act of effort comparable to training for an athletics event only indicates how low standards of achievement have sunk. People should be expected to grow a spine and take responsibility for their decisions as a matter of course, not pandered, patronised and praised for minor acts of agency like a toddler managing to eat his vegetables before his ice cream.
The supposed benefits of a month of abstention, apart from a “sense of achievement with your newfound hero status” — good grief — include losing weight, saving money and sleeping better. But one month out of twelve will not get you anywhere. If you are spending half of your life doing X and the other half worrying that you are doing too much of X, you are doing it all wrong. Either do less of X, or decide that the benefits of X are worth the costs. Do. Or do not. There is no try.
But maybe it will help to “beat cancer sooner”, and I should stop being a big meany. Well, it would be nice if Cancer Research UK would stop taking money away from its worthwhile research to squander on activism and lobbying.
The Dryathlon is, of course, just another bit of neo-puritan nagging. It probably makes a certain amount of sense for a cancer research charity to give out information that helps people balance fun versus risk. If I was told that my lifetime chance of getting cancer was 48% with total abstinence and 50% if I get completely drunk 3 times a week, and left it at that, I would say, “thank-you very much. Mine’s a pint of Pride.” But they will not do that. They’ll just tell me that alcohol causes 4% of cancer cases and really I should just stop thinking and drink less, and are happy to have taken a little bit of the joy out of the beer. Ok, it does not work on me but the BBC can find and interview people in a pub who have been made to feel bad about doing something they enjoy.
It does not stop there. Cancer research UK wants to prohibit product placement of alcohol. And in the latest pan–media offensive, we are told that there will be 700,000 cases of obese people getting cancer over the next 20 years, with no clue as to how significant this is. Then they are they are calling for a ban on advertising sugar before 9pm, a tax on sugary drinks, a general reorganisation of society to suit the NHS and, chillingly, the government to “take children’s health more seriously”. Supposedly children are bombarded with advertisments for sugary food and drink. I am a parent and I am not seeing it. I even have trouble buying sugary drinks without artificial sweeteners without resorting to Google and specialist suppliers.
I do not want to donate money to an organisation that is happy to goad the local mafia into “taking care” of me. Just cure cancer already so I can eat and drink what I want with impunity.
Here is a chart of average life spans for women from the Office of National Statistics with the dates replaced with letters. At some point on the X axis the National Health Service was created. Can you guess where? Answer below the fold.
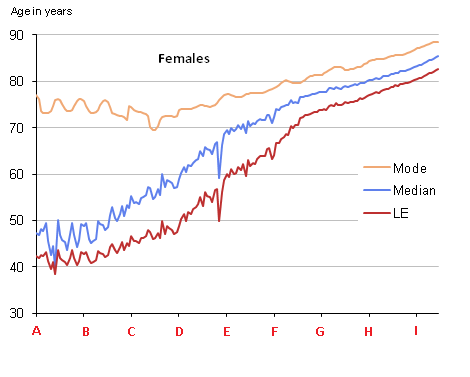
→ Continue reading: When was the NHS created?
A fourth-year medical student at Leicester University, Mr Ravindu Thilakawardhana, has been deemed unfit to practice medicine by the University, after making comments on Facebook towards someone who had annoyed him, the Independent tells us. It appears that he will not be permitted to complete his degrees and graduate, quite a long way down the line too.
Ravindu Thilakawardhana, who was in his fourth year studying medicine at the University of Leicester, became furious when a fellow student posted explicit pictures of his friend onto the social networking site.
Mr Thilakawardhana retorted with a photo of the actor Liam Neeson accompanied by the words: “I will look for you, I will find you, and I will kill you,” the Leicester Mercury reports.
He later sent a private message to the student saying: “I don’t want to see you on a night out in Leicester, or in the UK.”
The student reported Mr Thilakawardhana to the medical school who reprimanded him, before deeming him “unfit to practice medicine”.
The matter is going to law, with Mr Thilakawardhana taking legal action in the hope of having his sanction overturned.
There has been no criminal conviction (not even a prosecution) of Mr Thilakawardhana over his action, and yet his career is effectively ruined, as things stand, because of an intemperate post. This has all the hallmarks of a grotesque reaction to me.
How many other medical students might be barred from the closed shop profession for expressing attitudes that render them ‘unfit to practice medicine’? How wide might this ‘catch-all’ classification extend? Has all common sense left the University? (Yes, I know, by definition…) Is this not tyrannical, with echoes of Dr Bonham?
News reaches us that the NHS is considering blacklisting homeopathy in England, albeit at a glacial pace (with a consultation planned for 2016), by banning General Practitioners from prescribing homeopathic remedies.
I am tempted to suggest that the NHS merely dilutes the funding so much that it becomes more effective, but that would be facetious.
We are told that
…Drugs can be blacklisted if there are cheaper alternatives or if the medicine is not effective…
I am wondering how there could be a cheaper alternative to nothing?
And the Health Secretary, Mr Jeremy Hunt has chimed in, saying:
“when resources are tight we have to follow the evidence”.
One might hope that all clinical practice would follow the evidence whatever the state of resources.
Not all is lost (as it were) for adherents of homeopathy, as the proposal is limited to GP prescribing.
The result of the consultation would affect GP prescribing, but not homeopathic hospitals which account for the bulk of the NHS money spent on homeopathy.
What on Earth is a ‘homeopathic hospital’? A cemetery?
Could this be a small start in the battle against pointless government activity?
Christopher Snowdon’s Velvet Glove, Iron Fist: a history of anti-smoking does not make comfortable reading for libertarians. Although there were anti-smoking movements in the past by the beginning of the recent part of the story (roughly 1950) two principles reigned supreme: freedom of speech and personal responsibility. By the end both lay in tatters.
Snowdon comes from the position that smoking cigarettes is dangerous. This is a refreshing approach given that some libertarians are wont to deny this. Take, for instance, my good friend, the late Judith Hatton. In Murder a Cigarette, co-written with Ralph Harris of IEA fame, she argued that smoking is perfectly safe. Many was the time I would go round to her place for a free meal and be plied with cigarettes (as well as some food). Snowdon, on the other hand, is having none of it. Smoking is dangerous. It produces a chemical, benzo[a]pyrene, which messes around with DNA and causes lung cancer. He also has little time for the tobacco companies whom he regards as little better than scoundrels.
However, accepting that smoking is dangerous and that tobacco companies have been less than honest is his last concession to the anti-smoking lobby. As he says “the dose is the poison”. Heavy smokers are in trouble but light smokers not so much. Of all smokers, 10% will get lung cancer.
If I have a quibble it’s here. While Snowdon has plenty to say about smoking and lung cancer he has little to say about smoking and heart disease although he appears to accept the link there too. Given that heart disease is another big killer of smokers that is a bit of a shame. But anyway, adults should be allowed to make their own decisions for better or worse.
Sadly such appeals to individual choice cut little ice with the anti-smoking lobby. Over the years, they have campaigned for every type of restriction they can think of from advertising bans, to warnings on packs, to smoking bans in pubs and restaurants. One of the ironies is the ineffectiveness of the government violence they so cherish. Although research is sketchy, most restrictions, such as the ban on smoking in bars have had no obvious effect on the rate of smoking and in many cases seem to have increased it – at least initially. Another example is the ban on television advertising where again, initially, sales rose. The unintended consequence was to set in stone the market makeup at the date of the ban. Hence, while beforehand brands rose and fell, ever since Marlboro has been on top. Although Snowdon doesn’t say this as such the implication seems to be that the decline in smoking over the last 50 years has had little to do with government.
Particularly revealing is the search for technological solutions. Over the years the tobacco industry has introduced filters and low tar cigarettes. Whether these make much of a difference is unclear partly because little research has been carried out. Another brand experimented with palladium (just as you might find in a catalytic converter). Unfortunately, the advertising ban made it difficult for them to get the word around.
There were other problems with safer cigarettes. If the tobacco company marketed a safer cigarette as a safer cigarette that would imply that all the other cigarettes they had been selling were dangerous. That would be the sort of admission that could lead to them winding up in court. The tobacco companies were reluctant to admit this not least because, up to then, they had never actually lost a court case.
More recently we have seen the rise of vaping which is vastly safer. This has provoked a split in the anti-smoking lobby with some of them coming to the conclusion that if it comes to a choice between regulations and public health they are in favour of public health. This has not, however, prevented the introduction of a bunch of EU regulations which will make vaping more difficult.
But that is the exception. Generally speaking, the anti-smoking lobby has opposed these developments. They don’t want technological solutions. They want people to change their behaviour. It matters little to them whether lives are saved.
I can shed some personal light on this. A long time ago I was a green. (I know, I know, I was young and foolish.) Back then I utterly hated the idea of technological solutions to environmental problems. Quite why this was I really don’t know but to my green mind the only correct solution was for people to consume less.
Having proved that smoking was dangerous, the anti-smoking lobby then set out to prove that passive smoking was also dangerous. You can kind of see their point. If benzo[a]pyrene is dangerous then it should be so to any consumer of the smoke in which it is present. Snowdon looks at the studies in great detail but, as he shows, again and again they don’t prove anything of the sort. If anything, passive smoking is good for you. One study even suggested that children brought up in smoking families were less likely to get lung cancer.
But the anti-smokers weren’t about to let the facts get in their way. Repeatedly confronted with research that found no link between passive smoking and lung cancer they simply claimed the precise opposite. They were not even above smearing anyone including scientists who dared to point out that the facts were telling a different story. Any similarity between this and any other science which has been perverted by political chicanery is entirely coincidental.
But the campaign rumbled on and continues to rumble on regardless of the facts. My pet theory is what did for smoking is that it went from being an air freshener to being an air unfreshener. A hundred years ago, people’s nostrils would have been exposed to the foul odours caused by horse manure, industrial pollution, filthy rivers and coal dust. In such an atmosphere, cigarette smoke was at worst insignificant and in many cases an improvement.
The anti-smoking lobby has been so successful that recently it has had to start branching out. Alcohol, gambling, meat and sugar are now all on its radar screen of puritanical ire.
Keep bacon, abolish the World Health Organisation
– Roy Lyons
Monopolies are only sustained by force. Sometimes examples are useful.
In his book The No Breakfast Fallacy, Tim Worstall relates how in 2010 China limited the supply of rare-earth minerals to force the price up. The only problem was that rare-earth minerals are not rare at all, and the increased prices meant that Lynas Corporation and Molycorp were able to raise finances to re-open some mines that had been previously closed due to the previous low prices from China.
Today, Imprimis Pharmaceuticals announced that they are making for $1 an alternative to the drug Daraprim, in direct response to Turing Pharmaceuticals increasing its price from $13 to $750.
Update: Tim Worstall wrote about the Daraprim and rare-earths in Forbes. I hadn’t seen it when I wrote this, honest!
Via JohnW and the rest of the internet,
Treat meat eaters like smokers, warns Jeremy Corbyn’s new vegan farming minister Kerry McCarthy
(Just a little note to the Telegraph subs: she isn’t actually farming minister yet. Labour would have to win an election for that.)
Meat should be treated like tobacco with a public campaign to stop people eating it, Jeremy Corbyn’s new vegan shadow farming minister has suggested. Kerry McCarthy, MP for Bristol East, has irked the British farming industry with her veganism and vice presidency of the anti-hunting League Against Cruel Sports.
In an interview with Viva!life, a magazine for vegans, she admitted she was a “militant” when it came to clamping down on meat consumption. She said: “I really believe that meat should be treated in exactly the same way as tobacco, with public campaigns to stop people eating it.”
The Scottish and the Welsh NHS are the closest thing to a counterfactual, because they are still more or less run like the old (and, if the Corbynistas get their way, the future) English NHS. Even though they are, in per capita terms, better funded and generally better staffed than their English counterpart, their performance lags on most measures. Rates of mortality amenable to healthcare are higher than in England, waiting times are longer, and hospital infections are more prevalent.
– Kristian Niemietz
Eric Raymond is the reason I’m here. He’s the guy I found while learning about Linux who gave a name to my vague sense of injustice at having to pay tax and taught me that a libertarian is a thing. Googling “libertarian UK” after reading his web site is how I found Samizdata, and found out that there were libertarians on my doorstep. He taught me that anarcho-capitalism is a thing. And that it’s okay to like guns. And that it does not make me some sort of lefty for enjoying messing about with Free Software. He explained the economics of it and gave it a better name: Open Source. And he’s out there propagandising, and making some of the software that keeps civilization ticking and not being hacked. And his code is all over the place and you probably use quite a lot of it every day.
But he has a problem.
First, Obamacare killed my wife’s full-time job and the health insurance that came with it. Then Obamacare drove personal health insurance costs into the stratosphere, so I now pay more per month on it than I do for my mortgage. $973 a month is what it costs us to go to a doctor, which is ridiculous and every politician who voted for this disaster should be hung from a lamppost. Until it’s repealed or collapses, though, the money has to come from somewhere.
You get more of the things you encourage. I think ESR needs to be encouraged. And luckily, you can, via his Patreon page.
Also, on his blog post about Patreon, there is some interesting discussion about Obamacare:
Petro says:
People are shocked when I tell them what the “bronze” plan costs a family of 4 for insurance that has insane deductibles (it looks like they went up to 5k/person 10k/family) they are shocked.
PapayaSF adds:
It’s darkly ironic that one of the original arguments for Obamacare’s outlawing of inexpensive “junk insurance policies” was that many had deductibles that were “too high.” So now we’ve got expensive policies with high deductibles that are too high…
ESR explains his wife’s job loss:
The short version is that Obamacare mandates have added so much to an employer’s overhead for anyone full-time that the full-time job is being effectively abolished. Even professionals like lawyers are being fired to be replaced with contractors who have to buy their health insurance a la carte.
It’s a double whammy – first Obamacare destroys secure employment, then it saddles people living hand-to-mouth with ruinously high costs. Our health-insurance premiums are higher than our mortgage.
I don’t usually find much to sympathise with over at the Bella Caledonia blog. This account by Jonathan Rowson, whose brother has been committed to a psychiatric ward, was an exception:
Smoking and the Forbidden Garden – a Dereliction of Sanity?
Defending the rights of the mentally ill to do something that harms them is not a popular cause, but this much needs to be said: preventing psychiatric patients from smoking on hospital grounds is inhumane.
I am responding to the situation in a particular ward in a hospital in NHS Grampian region. At the time of writing my forty year old brother Mark is there, as he has been before. He is surrounded by other adult patients, many of whom are thought disordered, dysfunctional, and up to their eye balls in medication. Mark has given me permission to write publicly about his situation, but he is not well enough to grasp the full context. I am taking the liberty of making the following case on his behalf.
Many psychiatric patients are habitual smokers, but at the moment they are strictly not allowed to smoke anywhere on hospital grounds. Smoking has been banned in hospital buildings for about a decade, but in the hospital in question secure gardens adjacent to the locked wards and smoking shelters within the general grounds of hospitals were available to smoke. This arrangement seemed to work until the authorities decreed that the shelters should be knocked down and the secure gardens should be smoke free. Some psychiatric patients, staff and visitors now face the mild stigma and hassle of having to escape the hospital to smoke, but if you are sectioned under the mental health act it’s not so simple. The hospital ward is your de-facto home, and also your de-facto prison, so where do you go?
The ruling is unenforceable. In fact most staff feel they have no choice but to turn a blind eye. Patients are now smoking in their rooms or in the bathrooms; anywhere where the staff can have plausible deniability of not seeing them. Alas, the collateral damage of this necessary open secret is that none of the patients can now go to the outdoor area assigned to the ward. The small secured gardens are the most humanising place on the ward and a vital source of fresh air, but they lie unused due to the risk, not that patients will smoke, but that they will be seen to be smoking, and get staff into trouble as a result.
Most of the comments are supportive, but not all. This one by Clive Scott was notable for its self-righteousness:
What about the employer’s responsibilities to provide a safe working environment for employees and the rights of non-smokers for wholesome air? It would be ridiculous to permit the mentally enfeebled to flout regulations for the common good simply because of their illness. Smoking is a disgusting foul habit and addiction and every step possible should be taken to eliminate it from society.
Scientists find mutation that protects against ‘mad cow’ disease after studying cannibal group
Scientists have found a genetic mutation that imparts complete protection against the human form of “mad cow” disease, which could lead to new ways of tackling similar incurable brain diseases.
The researchers discovered the mutation after studying the genes of the Fore people of Papua New Guinea who until recently had practised a form of cannibalism where a related disease was transmitted by eating the brain tissue of the dead.
[…]
At the height of the kuru epidemic in the mid-20th Century, the disease was killing about 2 per cent of the Fore population every year. Some villages had become so severely depopulated they risked dying out, with few if any women of child-bearing age left alive.
However, the scientists believe that people who had been born with the resistance mutation may have helped to re-populate the Fore villages, leading to a rise in the number of individuals who were resistant to kuru.
If I had more brains my first thought on reading this article in the Independent would have been, as it was for Professor John Collinge, director of the Prion Unit:
“This is a striking example of Darwinian evolution in humans – the epidemic of prion disease selecting a single genetic change that provided complete protection against an invariably fatal dementia.”
But if I had more brains I wouldn’t need a second thought.
|
Who Are We? The Samizdata people are a bunch of sinister and heavily armed globalist illuminati who seek to infect the entire world with the values of personal liberty and several property. Amongst our many crimes is a sense of humour and the intermittent use of British spelling.
We are also a varied group made up of social individualists, classical liberals, whigs, libertarians, extropians, futurists, ‘Porcupines’, Karl Popper fetishists, recovering neo-conservatives, crazed Ayn Rand worshipers, over-caffeinated Virginia Postrel devotees, witty Frédéric Bastiat wannabes, cypherpunks, minarchists, kritarchists and wild-eyed anarcho-capitalists from Britain, North America, Australia and Europe.
|



